This was originally published here, in French (link).
We provide this translation for your convenience. Practical aspects may differ where you live.
I'm switching to 1/17
by Charles-Edouard!
There are so many and more! Silence radio side effects... And here is one who complains (how dare he) that DTG (in monotherapy...) makes him fat, and starts a concert of Me-Too, Me-Too, Me-Too. They could have a little bit of recognition of the belly! The 4/7 (lousy...) and the mono-DTG (at 50 mg all the same!), was not invented by them: if we hadn't told them about it, they wouldn't have been interested... Thank you for the information, and here I am, enjoying it and forgetting to share it with others...We have to talk about these things, otherwise it gets forgotten...
It's the 17th of the month: I'm going for it!

Leibo told me that he would have considered it, but that it meant 'playing gymkhana with the Republican calendar'. Well yes, you better have an Excel spreadsheet, a calendar to mark and alarms on your smartphone! To keep up with 1/8, 1/9, etc. It's the progressive method, it's a good method: it reduces the risks.
Well... At 1/15, you take a break, because the motivation disappears as well as the discomfort and the side effects. At 1/15, you are safe and relaxed... But now, the 1/30 is tickling me again, especially since the appearance of injectables, the only serious competitor.
New schedule, new notation: 1/17 = 1/16/1/13
Here is my new idea to solve the 'gymkhana of the republican calendar'. The 1/15 means one take on the 1st of the month and one on the 15th, and here we go again. The first day of the month is by far the easiest: it's the day you have to give back your expense report: don't forget it... If you don't, the accounting lady will be all over you! So, on a fixed date, you do the accounting, the papers, etc. Taking your meds is just another item on the list: no need for an alarm, it's automatic. The 15th is another matter! There you have the alarm on the smartphone, the automatic email that reminds you: no way to forget!
If you think about it, the 1/15 is one alarm per month, that's all! I've never missed it. Don't mess around, this is serious. The 1/15 is cool, not very intrusive, but you mustn't forget.
And you're back on your feet on the 1st of the following month. At 1/17 you'll be playing the big game: you have to plan ahead, and the comfort of the first of the month is over! Fortunately there is a trick!
On the 15th, you have your alarm, and on the 1st not really. Between the first of the month and the first of the following month, there is something in the middle. What if we shift this point without touching our monthly appointments...
the 1/17 followed by a 1/13: we get back on our feet
The sequence is: 1 dose, 16 days break, 1 dose, 13 days break. It is very easy to do. Just shift the 15 th to the 17 th.
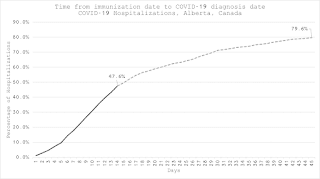
What is the benefit? None on the consumption of drugs, on the Freedom day (which remains Jan. 24). The idea is to use the OFF window to enlarge the Eclipse, which I lost the vision of. With a weak but present reservoir I had an Eclipse of 27 days. Today, I don't have any reservoir or PCR at hand.
Grail researchers (Ananworanitch, Siliciano, ...) tried it: nobody succeeded anything. I proposed a strategy during my conference at Pasteur, and... I followed it and I have the best results ever! Voilà!!!
The 1 over 8
Well... I must admit that the 2/7 and other 1/7 are already in the ecstasy of their 'performance'. Yet... So far from the goal, so far from the Monster, it is a relative performance: Yes, it is better what is being done at Bichat and consort. Above all, we can do better. To do it in comfort? Why not shift a day, occasionally, check, make sure, move forward! Once, from time to time, then more often, shift to Tuesday, (or even Wednesday, etc.), even if it means resuming your senatorial rhythm the following Monday. Just a suggestion...
In Memoriam... Jacques Leibowitch

I have been informed that some would like to set up archive interviews with people who have crossed and contributed to his story. They would like to know if I agree, to tell how I met him, collaborated with him etc. .... Yes! with pleasure!
In fact, I only met him 5 or 6 times. He was using mail a lot and I learned a lot. He is the one who taught me the concept of the Eclipse, first explained by P. Sonigo. The idea to make a Council of the Eclipse is an old idea of Leibowitch. I would like to ask Sonigo and others about it...
I also have in mind that we could create a Leibowitch Prize to salute and encourage the wide adoption of his ideas throughout the world...
Pieces of Anthology

One cannot say that Molinar has been especially brilliant in this crisis!...
One could also extend the compliment to the poor knowledge that pharmacologists (cf Peytavin and others...) have of RetroViral biology. It is also true that this biology, so important for us, deserves to be better exposed... When will Sonigo make a video on this subject where he excels?
In the news

This study has a transparent and unequivocal triple message:
1) statins have no clinical utility (efficacy);
2) lowering bad cholesterol has no clinical utility;
3) cholesterol is innocent in cardiovascular disease.
If I add that these drugs are highly toxic ....
- Moderna announces working on mRNAs for other pathologies Press release. Including HIV... We'll see...
The French genius

I was in pursuit of a fantasy, of an impossible (re)incarnation, of a Faustian pact. I would give body and soul (especially the body....) to enter that of... The Evangelist... It's something I wish I knew how to do, almost to the exclusion of everything else. And for me, the best Evangelist is in the St. Matthew Passion (where I excelled moderately), in Sir Simon Rattle's version in Berlin. You can get a free access, here, on the Philharmonie website.
Mark Padmore excels there... However, if you look a little further, you will find this little gem, a composition by the Frenchman Hahn, sung by an English tenor: a serenade in Italian. Unexpected and definitely adorable. It has already 3000 views! What a worldwide success! It's in the soundtrack of a movie that looks very nice too: The Man in the Hat, see trailer here.
Padmore's version (You Tube) is the only one I'm excited about. Under its title La Barcheta (Venezia) one finds several versions of it of which one as remarkable as aged: a Barcheta sung by R. Hahn himself! One plunges in the time... From Hahn you can try this piece on the piano, A Cloris.
There is also this (amateur?, Mexican?) version of the Barchetta by a tenor in training. It is remarkable for its authenticity!(190 views, after all!) And we enjoy remembering this sublime Italian lover, so loved and our games under the changing shadows of the Baths of Caracalla ... Delicious!
Feel free to comment, like, share and use
Turn off the TV and don't be fooled by the Parisian venality